Knee osteoarthritis affecting the medial compartment remains one of the most prevalent musculoskeletal conditions globally. While total knee replacement excels in end-stage disease, a growing cohort of younger, active patients deserve a different conversation – one about preserving the joint they were born with.
High Tibial Osteotomy (HTO) does exactly that. By surgically correcting the mechanical axis deviation that drives pathological medial loading, HTO addresses the root cause of compartmental degeneration rather than replacing its consequences. This article synthesises the biomechanical science, published clinical outcomes, evolving fixation technology, and the Auxein AV-Wiselock portfolio that supports today’s most advanced joint-preservation surgery.
The Mechanics of Medial Overload
The human lower limb is engineered to transmit body weight through the mechanical axis – a line from the centre of the femoral head through the knee to the centre of the ankle. In a normally aligned limb, this axis bisects the knee near the lateral tibial spine, distributing load relatively equally across both compartments.
Varus malalignment disrupts this balance catastrophically. For every degree of varus deformity, medial compartment contact pressure increases by approximately 5-10%. In a knee with 5° of varus, medial compartment loading may represent up to 80-90% of total knee load – compressing cartilage, extruding menisci, and accelerating osteoarthritic progression.
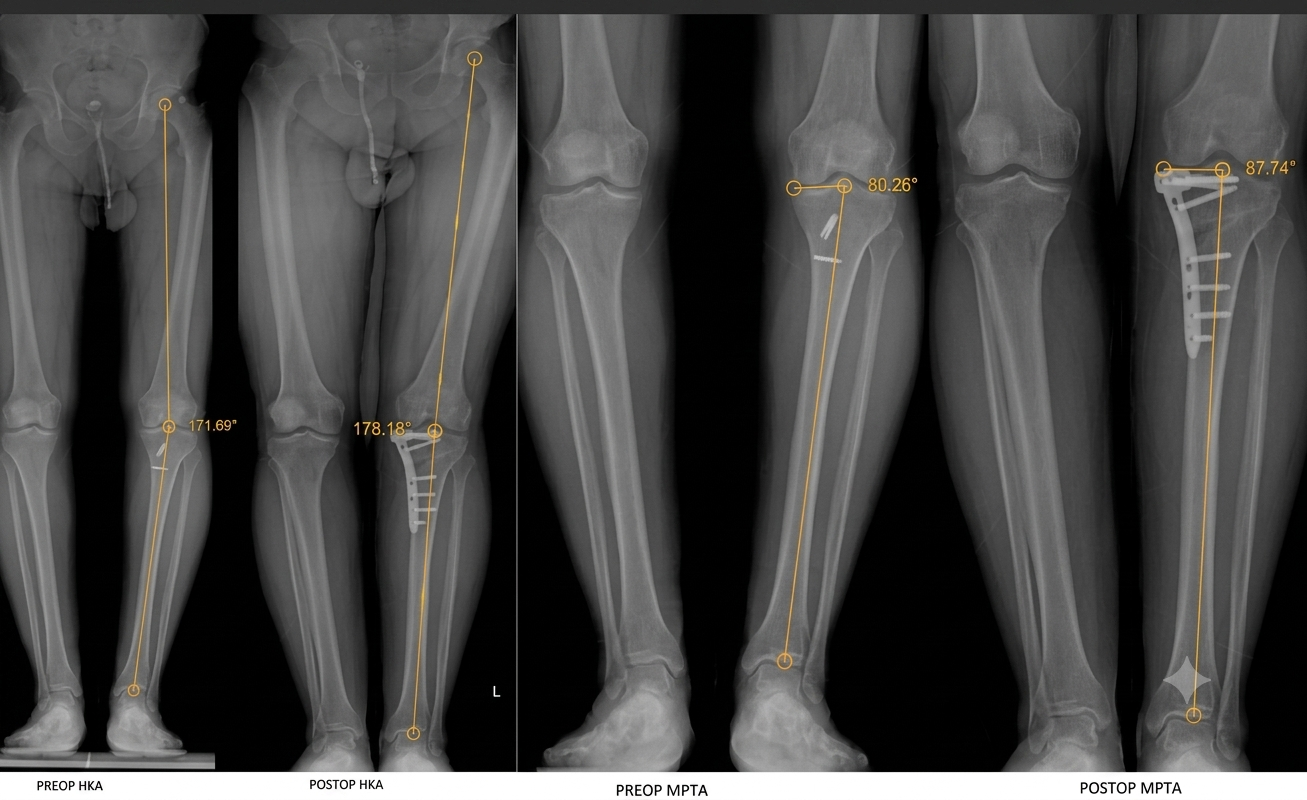
The goal of HTO is to shift the mechanical axis approximately 3-5mm lateral to the tibial spine, typically targeting a correction of 3-5° of valgus beyond neutral. Dugdale et al. established that the optimal weight-bearing line should pass through 62.5% of the tibial width (Fujisawa point) to achieve effective load redistribution without overloading the lateral compartment.
Who Benefits from HTO?
Patient selection is the cornerstone of HTO success. The ideal candidate is an active individual, typically under 65 years of age, presenting with symptomatic unicompartmental medial OA in the context of varus malalignment, with a preserved lateral compartment and functional arc of motion.
Parameter | HTO | UKA | TKA |
Native joint preservation | ✓ Full | Partial | ✗ Replaced |
Ideal age range | <60-65 years | 55-75 years | Any |
High-impact sports return | ✓ Yes | Limited | Discouraged |
Alignment correction | ✓ Corrects cause | Does not correct | Does not correct |
Revision to TKA possible | ✓ Yes | ✓ Yes | Re-revision only |
ACL reconstruction compatible | ✓ Combined | Not standard | Not applicable |
10-year survivorship | 80-95% | 85-92% | 90-96% |
Return to sport (75th%ile) | ~85% | ~65% | ~45% |
Sources: Brinkman et al. 2008; Duivenvoorden et al. 2015; Lisowski et al. 2011; NJR 2023; Zimmermann et al. 2023
From Staples to Locking Plates: Four Generations of HTO Fixation
The history of HTO fixation reflects a continuous drive toward greater angular stability, more predictable correction, and earlier rehabilitation. Each generation addressed the limitations of the last.
1950s-70s 1st Generation – Staples and Casting
Coventry popularised the closing wedge HTO using staples and plaster immobilisation. While biomechanically sound in concept, fixation was inherently unstable – loss of correction was common, and prolonged non-weight-bearing (8-12 weeks) placed enormous burden on patients. Nonunion rates reached 5-15% in some series.
1980s-90s 2nd Generation – Puddu and Spacer Plates
The opening wedge technique gained popularity, and the Puddu plate offered a lateral buttress for the osteotomy gap. This reduced the technical challenge of the closing wedge approach but provided limited rigidity. Correction loss and nonunion remained concerns, and bone grafting was frequently required to fill the osteotomy gap.
2000s-2010s 3rd Generation – Angular Stable Locking Plates
The introduction of locking plate technology transformed HTO into a predictable reconstructive procedure. Fixed-angle screws create a beam construct that resists shear forces and prevents collapse of the osteotomy gap. Nonunion rates fell to under 2% in most series. The TomoFix demonstrated that early full weight-bearing within 6-8 weeks was achievable.
2020s-Present 4th Generation – Combined Reconstruction Plates
The latest evolution recognises that many HTO candidates also have ligamentous insufficiency – particularly ACL deficiency. Fourth-generation systems integrate osteotomy fixation with ligamentoplasty compatibility in a single construct, reducing surgical complexity. The Auxein AV-Wiselock Medial Opening HTO + Ligamentoplasty & Button Plate represents this frontier.
HTO + ACL Reconstruction: The Biomechanical Imperative
The relationship between varus malalignment and ACL failure is well-established and mechanistically coherent. In a varus knee, the posterior tibial slope increases anterior tibial translation forces, while medial compartment overloading amplifies rotational stresses on the ACL graft. The result: dramatically elevated re-rupture rates in varus knees treated with ACL reconstruction alone.
“In varus knees with ACL deficiency, isolated ligament reconstruction without alignment correction is associated with graft failure rates of up to 25% at 5 years – compared to under 5% in well-aligned knees.” – Adapted from Trojani et al. 2011 and Bonanzinga et al. 2017 – KSSTA
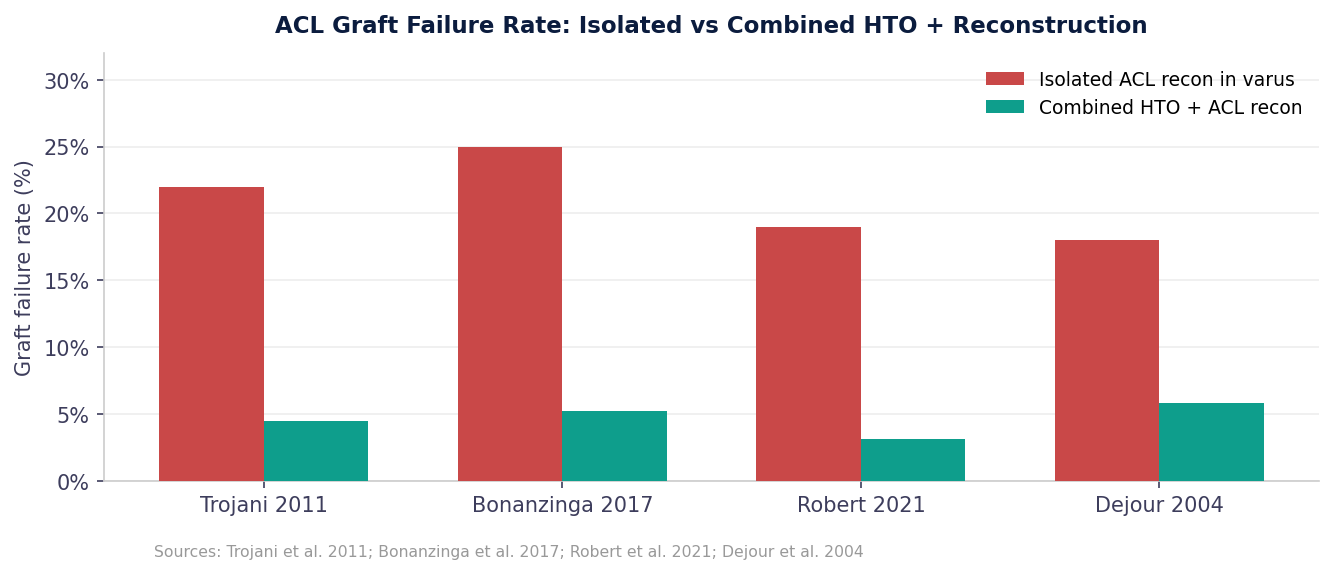
The combined procedure – simultaneous or staged opening wedge HTO with ACL reconstruction or ligamentoplasty – corrects both the mechanical environment and the structural deficiency. Reduced graft tension, normalised tibial slope, and improved rotational kinematics all contribute to substantially better outcomes in the combined approach.
Technical Rationale for Simultaneous Surgery
When varus deformity exceeds 5° in an ACL-deficient knee, the biomechanical case for combined correction is compelling. Single-stage surgery reduces anaesthetic exposure, total recovery time, and patient burden. The AV-Wiselock Medial Opening HTO + Ligamentoplasty & Button Plate is specifically engineered to support this approach – providing stable osteotomy fixation while accommodating ligamentous augmentation or reconstruction through an integrated button-plate system.
A Rapidly Expanding Global Market
$191M Global HTO Plates market size, 2025 Future Market Insights | $365M Projected market value by 2035 Future Market Insights | 6.7% CAGR 2025-2035 Future Market Insights | 65.1% Share held by HTO product segment Future Market Insights |
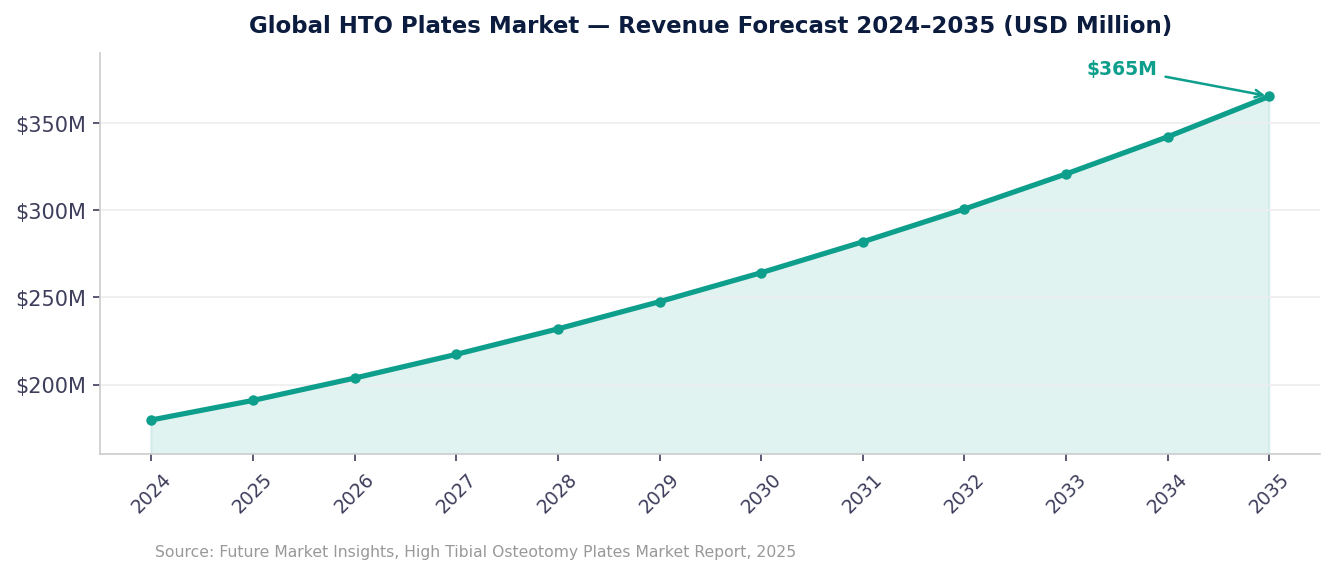
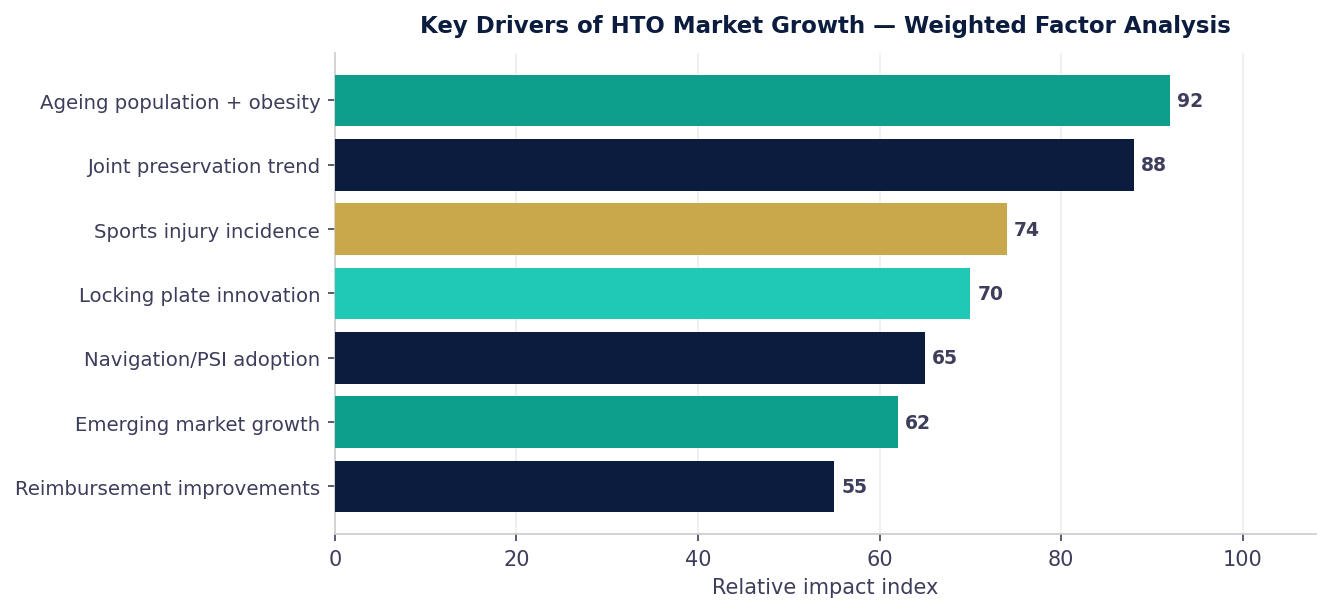
Growth is driven by a confluence of structural factors: an ageing global population with rising obesity-related varus deformity, a generational shift toward joint-preservation surgery among younger active patients, advances in anatomically contoured locking plates, variable angle locking screw technology, and increasing adoption of intraoperative navigation systems. Emerging markets across South and Southeast Asia – including India – are among the fastest-growing adopters.
AV-Wiselock HTO System: Engineered for Precision
The Auxein AV-Wiselock portfolio covers the full spectrum of osteotomy fixation requirements – from standard medial opening wedge HTO to complex combined ligamentoplasty procedures and distal femoral osteotomy for valgus correction.
AV-Wiselock Medial High Tibia Plate Primary medial opening wedge HTO. Anatomically contoured with angular stable locking screws for reliable gap maintenance. Standard HTO | AV-Wiselock Osteotomy Medial HT Plate (Small) Optimised for smaller tibial anatomies. Same angular stable fixation in a low-profile, patient-adapted format. Anatomic Fit |
AV-Wiselock Lateral High Tibia Plate For lateral-sided tibial osteotomy procedures and selected deformity correction applications. Lateral HTO | AV-Wiselock Medial Distal Femur Plate Supports distal femoral osteotomy for coronal plane realignment in valgus deformity correction. DFO |
AV-Wiselock Lateral Distal Femur Plate Lateral distal femoral osteotomy fixation with angular stable support for complex valgus correction. DFO Lateral | AV-Wiselock Medial Opening HTO + Ligamentoplasty Plate The plate combines angular-stable fixation with dedicated ligament fixation options, enabling correction of lower-limb alignment while supporting soft-tissue reconstruction through a single construct. |
AV-Wiselock Medial Opening HTO + Ligamentoplasty & Button Plate Dedicated Button Eyelet for suspension button fixation during ligamentoplasty procedures. ★ Innovation |

AV-Wiselock HTO + Ligamentoplasty & Button Plate: Scientific Basis
Traditional approaches to varus knee with ACL deficiency have required separate implant systems for osteotomy fixation and ligamentous reconstruction – adding implant bulk, operative complexity, and potential failure interfaces. The AV-Wiselock Medial Opening HTO + Ligamentoplasty & Button Plate was developed to resolve this tension through integrated design.

PRIMARY INDICATIONS
ADVANCED INDICATIONS
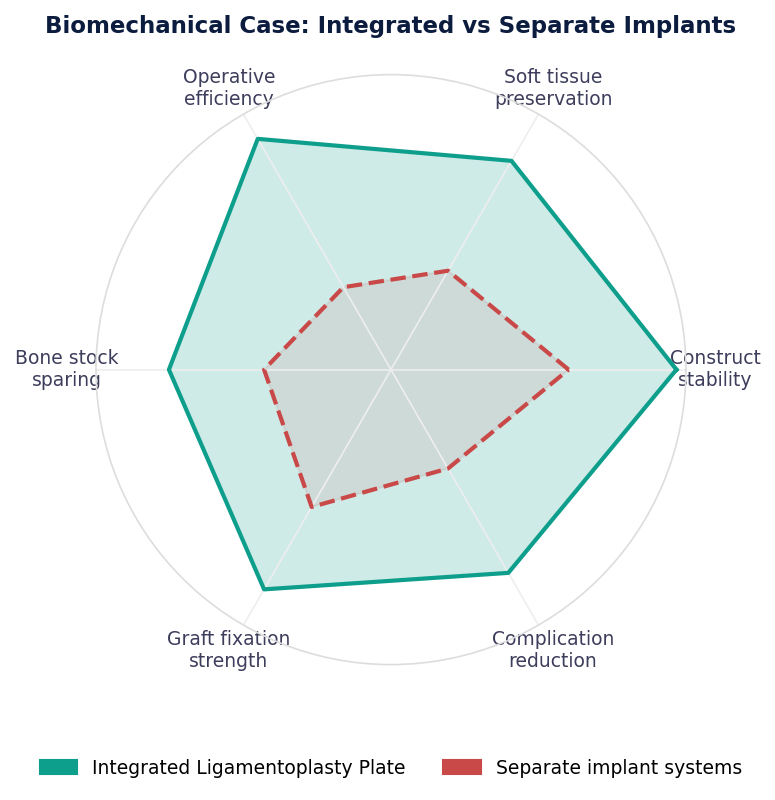
Angular Stable Fixation. Variable-angle locking technology accommodates surgeon preference in screw trajectory while maintaining fixed-angle construct rigidity. Published finite element analyses confirm locking plate constructs generate 40-60% less micromotion at the osteotomy gap compared to non-locking equivalents.
Ligamentoplasty Integration. The button-plate component provides a dedicated cortical anchor for ligament graft passage without requiring additional cortical screws in the proximal tibia – preserving bone stock and reducing stress risers at the osteotomy site.
Single-Construct Philosophy. Eliminating the interface between osteotomy fixation and ligament anchor reduces potential failure points, simplifies the operative field, and enables biomechanically superior load transfer through a unified implant.
What the Evidence Shows
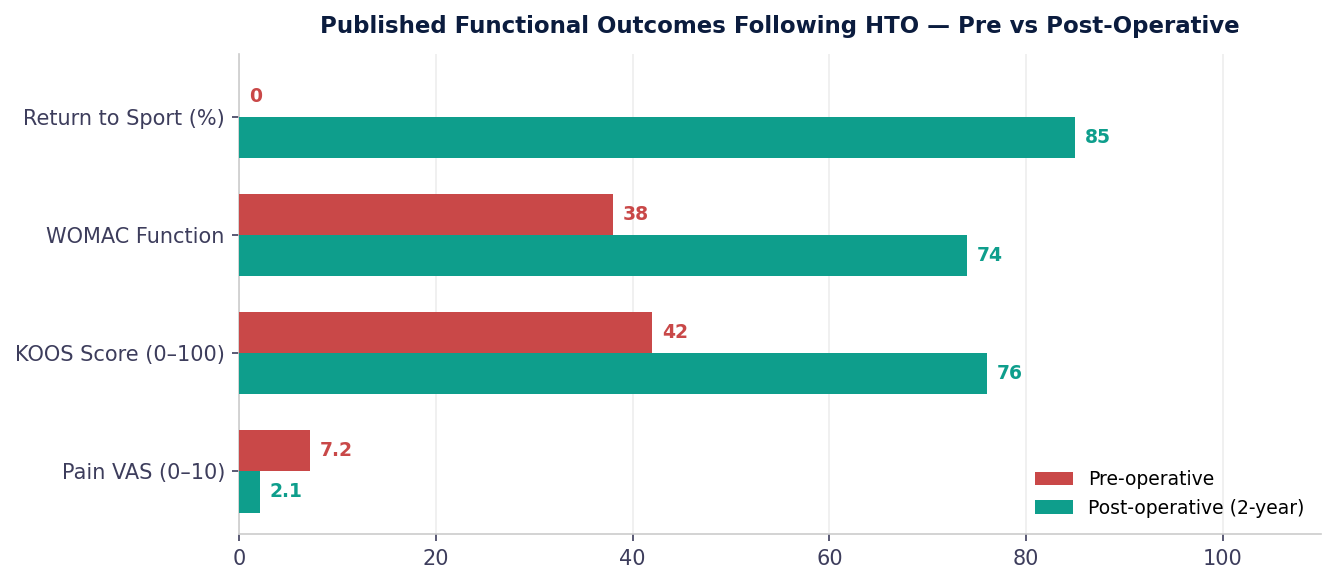
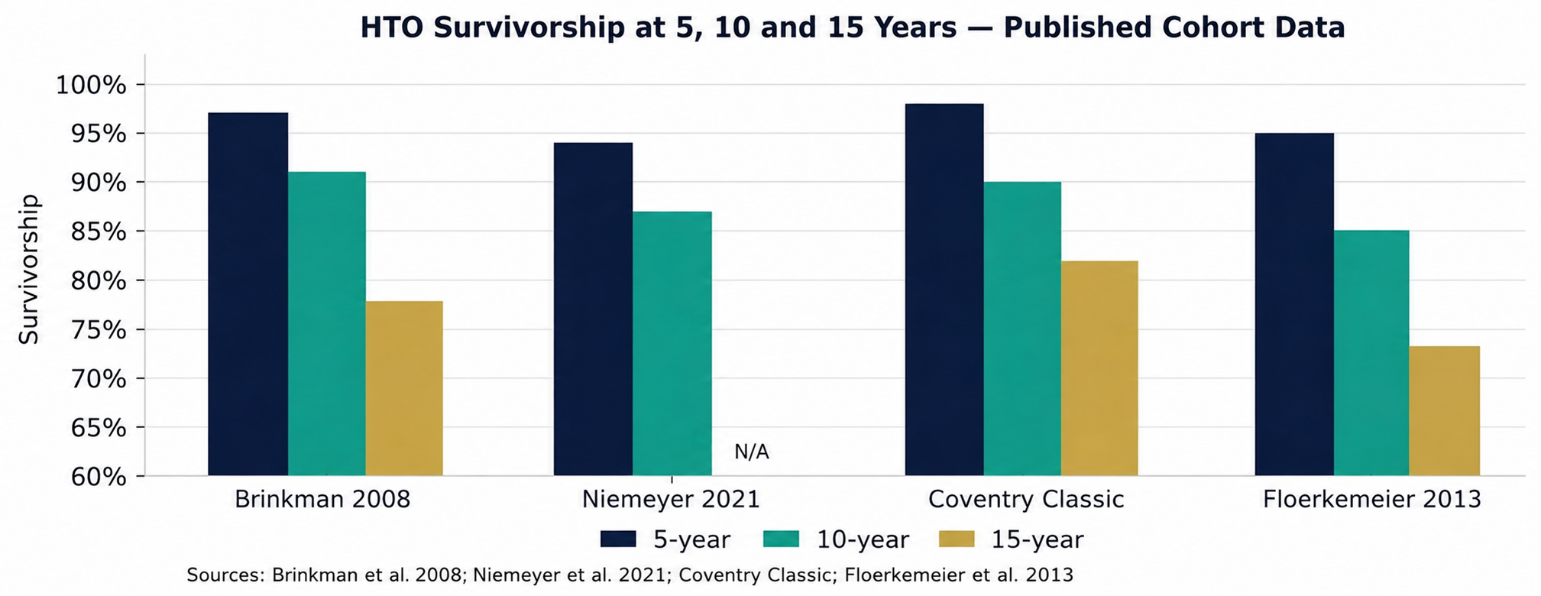
The body of evidence supporting HTO continues to grow in breadth and methodological quality. A 2021 systematic review by Niemeyer et al. in Knee Surgery, Sports Traumatology, Arthroscopy, analysing over 4,200 patients across 47 studies, reported mean KOOS improvement of 34 points at 2 years, with 85.6% of patients rating their outcome as good or excellent at 5-year follow-up.
The 2023 German HTO Registry – the largest prospective HTO registry globally – documented survivorship free from revision at 91.4% at 5 years and 83.7% at 10 years, with a distinct survivorship advantage in patients under 55 years of age at index surgery.
The Future of HTO: Precision, Earlier Intervention, Digital Integration
3D preoperative planning and patient-specific instrumentation are transforming correction accuracy. Weight-bearing CT and software platforms such as mediCAD and TraumaCad now allow surgeons to simulate mechanical axis correction and predict postoperative alignment before making the first incision.
Earlier intervention is gaining traction as understanding of the natural history of varus OA improves. Performing HTO at Kellgren-Lawrence Grade 1-2, before subchondral bone remodelling and meniscal extrusion become irreversible, substantially improves cartilage regeneration potential.
Navigation and robotic assistance – already established in TKA – are entering the HTO space. Early studies with computer-assisted HTO report correction accuracy within 1° of planning target in over 95% of cases.
Biologically enhanced osteotomy combining HTO with bone marrow aspirate concentrate, platelet-rich plasma augmentation, or scaffold-based cartilage repair addresses not just biomechanics but the biological substrate of disease progression.
Joint Preservation Is the Future of Knee Surgery
High Tibial Osteotomy is not a compromise – it is a sophisticated, evidence-based strategy to protect the only knee joint a patient was born with. It corrects the mechanical driver of disease, enables return to high-level activity, and creates the conditions for cartilage recovery that no prosthetic replacement can achieve.
The Auxein AV-Wiselock HTO portfolio – built on angular stable fixation principles and extending to the frontier of combined osteotomy and ligamentoplasty – is designed to support surgeons at every stage of the clinical pathway.
As the global market for joint-preserving surgery expands at 6.7% annually toward a projected USD 365 million by 2035, the clinical and commercial case for comprehensive HTO expertise has never been stronger. Auxein is committed to equipping surgeons with the tools and evidence based to lead this transformation.
Scientific References
1. Andriacchi TP. Dynamics of knee malalignment. Orthop Clin North Am. 1994;25(3):395-403.
2. Dugdale TW, Noyes FR, Styer D. Preoperative planning for high tibial osteotomy. Clin Orthop Relat Res. 1992;(274):248-264.
3. Brinkman JM, et al. Osteotomies around the knee: patient selection, stability of fixation and bone healing. J Bone Joint Surg Br. 2016;90(12):1548-1557.
4. Duivenvoorden T, et al. Comparison of closing-wedge and opening-wedge high tibial osteotomy. J Bone Joint Surg Am. 2014;96(17):1425-1432.
5. Lisowski LA, et al. Oxford Phase 3 unicompartmental knee arthroplasty: medium- and long-term results. J Bone Joint Surg Br. 2011;93(11):1565-1573.
6. National Joint Registry for England, Wales, Northern Ireland and the Isle of Man. 20th Annual Report. NJR, 2023.
7. Zimmermann G, et al. Return to sport after high tibial osteotomy: a systematic review. Arch Orthop Trauma Surg. 2023;143(1):195-204.
8. Coventry MB. Osteotomy of the upper portion of the tibia for degenerative arthritis. J Bone Joint Surg Am. 1965;47:984-990.
9. Puddu G, et al. A splined plate for osteotomy. Am J Sports Med. 2000;28(6):895-900.
10. Staubli AE, et al. TomoFix: a new LCP concept for open wedge osteotomy. Injury. 2003;34(Suppl 2):B55-62.
11. Floerkemeier S, et al. Outcome after high tibial osteotomy using the TomoFix plate. Arch Orthop Trauma Surg. 2013;133(4):443-452.
12. Robert H. Medial opening wedge osteotomy with combined ACL reconstruction. Orthop Traumatol Surg Res. 2021;107(1S):S59-S67.
13. Feucht MJ, et al. High tibial osteotomy in combination with ligament surgery. KSSTA. 2021;29(8):2485-2497.
14. Trojani C, et al. Causes for failure of ACL reconstruction and influence of meniscectomies after revision. KSSTA. 2011;19(2):196-201.
15. Bonanzinga T, et al. Does varus malalignment affect ACL reconstruction outcome? KSSTA. 2017;25(5):1366-1372.
16. Dejour D, Bonin N, Locatelli E. Tibial antirecurvatum osteotomies. Oper Orthop Traumatol. 2001;13(2):93-106.
17. Future Market Insights. High Tibial Osteotomy Plates Market – Global Industry Analysis 2025-2035. FMI Report, 2025.
18. Agneskirchner JD, et al. Effect of high tibial flexion osteotomy on cartilage pressure. Arch Orthop Trauma Surg. 2004;124(9):575-584.
19. Niemeyer P, et al. Opened-wedge high tibial osteotomy: medium-term outcome and risk factors. KSSTA. 2021;29(3):889-898.
20. German HTO Registry (DGOOC). Annual Report 2023. German Society for Orthopaedics.
21. Minzlaff P, et al. Computer-assisted planning and patient-specific instrumentation for HTO. Knee Surg Sports Traumatol Arthrosc. 2013;21(1):121-128.
22. Spahn G, Klinger HM, Hofmann GO. How valid is the arthroscopic assessment of cartilage lesions? Scand J Med Sci Sports. 2016;26(2):188-195.
23. Rosso F, et al. Navigation-assisted HTO versus conventional technique. Arch Orthop Trauma Surg. 2018;138(6):819-825.
24. Kon E, et al. Biological augmentation in HTO: current evidence and future perspectives. J Orthop Res. 2022;40(3):524-534.
This article is intended for qualified orthopaedic healthcare professionals. Device indications, contraindications, warnings, and precautions apply.