Pelvic fractures represent some of the most severe injuries in trauma care, often associated with high morbidity and mortality due to hemorrhage, instability, and concomitant visceral injuries. The evolution of pelvic plating systems and adjunctive devices like the Pelvic C clamp has significantly improved outcomes.
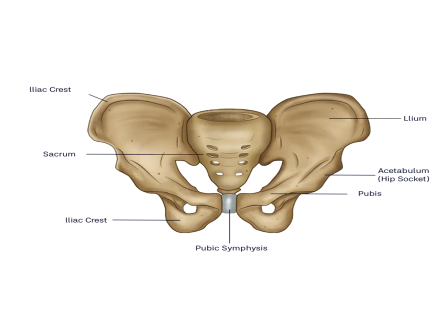
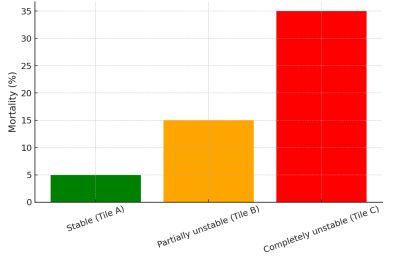
The pelvis acts as the keystone of the axial skeleton, transmitting body weight to the lower limbs and supporting vital organs. Instability due to fracture disrupts load transfer, leading to shock and disability.
Evidence-based indications include:
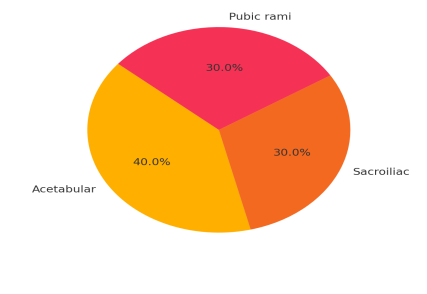
The Auxein Pelvic Plating System is designed for fractures, fusions, and osteotomies of the acetabulum, sacrum, ilium, and pelvic ring. It provides a comprehensive range of plates and screws tailored for pelvic and acetabular fractures. The system features: – Strategically contoured plates for precision.
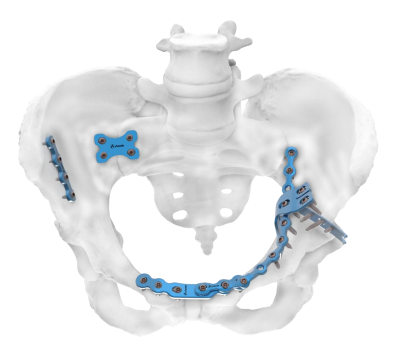
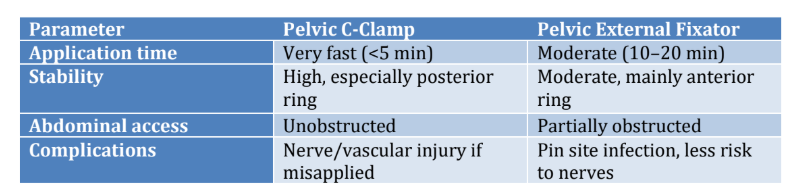
Pelvic plating systems, including the Auxein Pelvic Plating System, have transformed outcomes in pelvic fracture management. Combined with emergency stabilization techniques like the C-clamp, they provide life-saving benefits. Future trends point toward customized implants and damage-control orthopedics for improved survival and function.
US FDA 510k Cleared, CE Marked, MDSAP, ISO 13485:2016, EU-MDR 2017 certified
Indian FDA Approved | GMP Certificate
USA
Auxein Inc.
1500 Nw 89th Court, Suite 107-108,
Doral, Florida 33172
Tel: +1 305 395 6062
E Fax: +1 305 395 6262
Email: USoffice@auxein.com
Mexico
Auxein México S.A. de C.V.
Tepic 139 int 801, Colonia
Roma Sur,
Alcaldía Cuauhtémoc, CDMX,
México, C.P. 06760
Tel: +521 55 7261 0318
Email: info@auxein.mx
Dubai UAE
Auxein Medical Trading FZCO
Oud Metha Offices Building,
B Block 1st Floor Office No.26,
Near Healthcare City,
PO BOX-25572
Tel: +971 438 71333
Email: info@auxein.com
India
Auxein Medical Pvt. Ltd.
Plot No. 168-169-170, Phase-4,
Kundli Industrial Area,
HSIIDC, Sector-57, Sonepat – 131028,
Haryana
Tel: +91 99106 43638 | Fax: +91 86077 70197
Email: info@auxein.com