Understanding the Science Behind Pullout Resistance in Orthopedic Fixation
In orthopedic fixation, construct failure rarely originates from implant metallurgy alone. More often, failure begins at the bone-implant interface – where inadequate purchase, poor bone quality, or unfavorable force distribution compromises stability. Screw divergence has emerged as a compelling, biomechanically grounded strategy to address this challenge. But does angled fixation truly improve pullout strength?
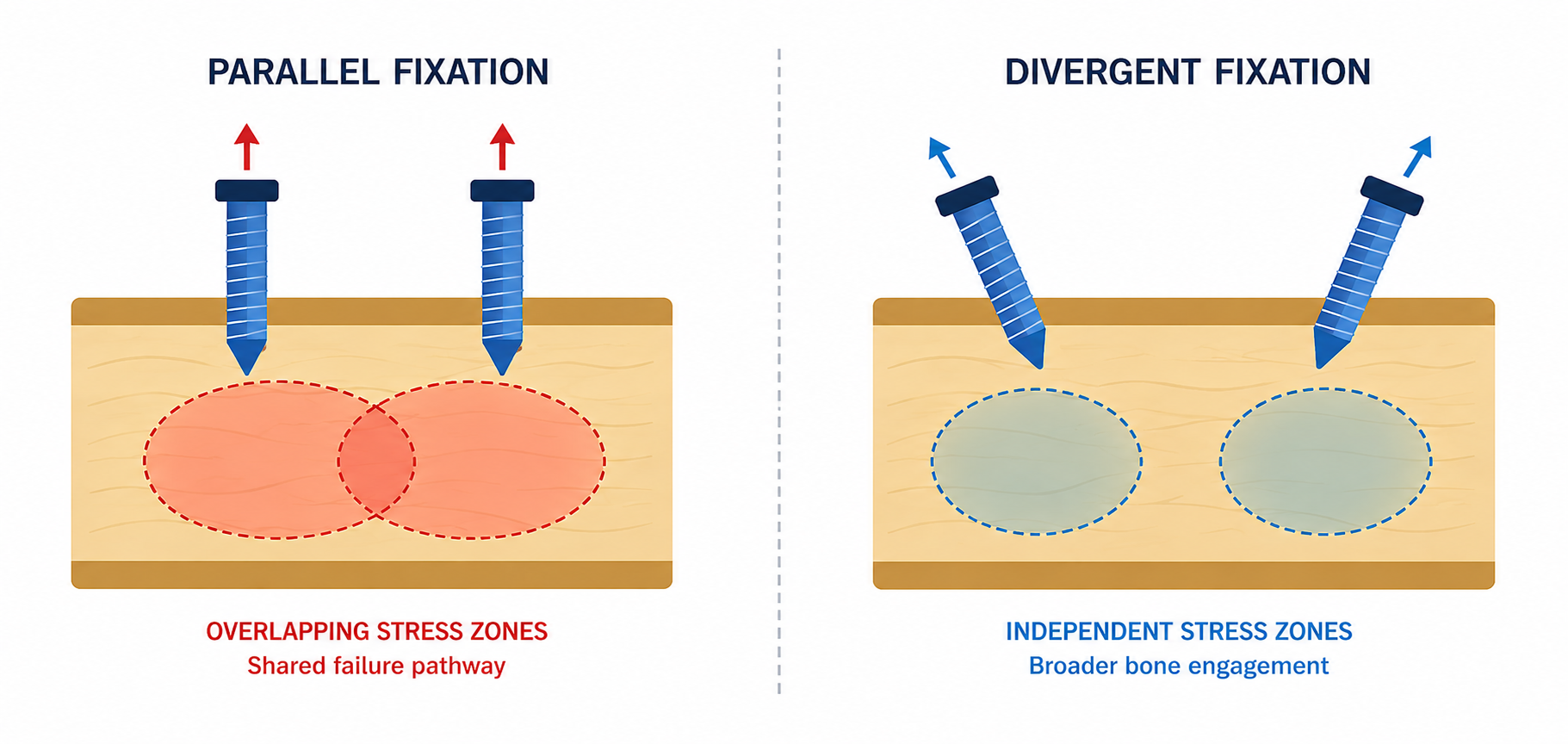
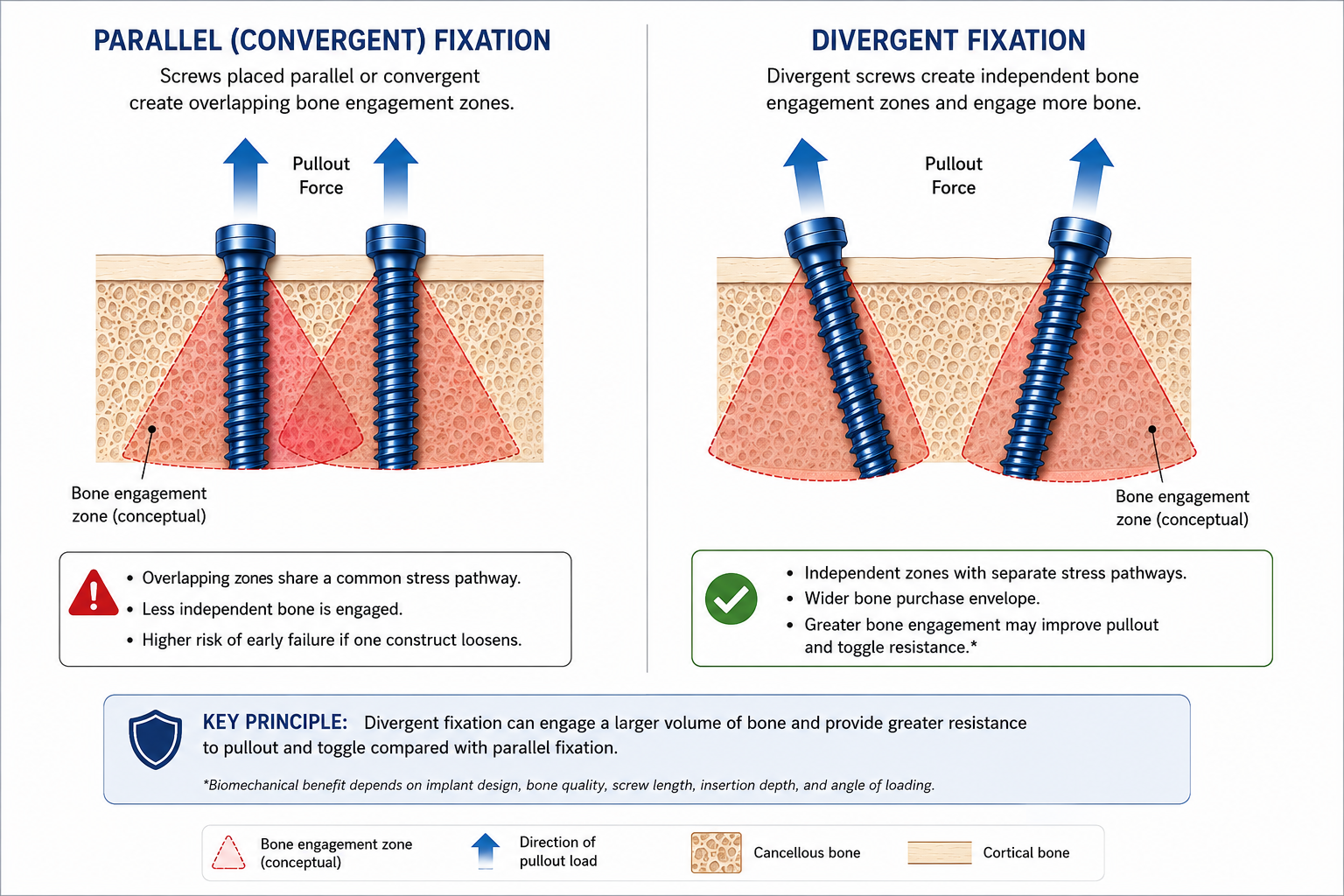
The pullout strength of any screw construct depends on the volume and quality of bone engaged by the threads, the length of engagement, and the distribution of stress around the implant. When screws are placed in parallel, their individual stress cones-the conical regions of bone that resist axial pullout-overlap substantially. This overlap means that both screws may fail along the same bone pathway simultaneously, creating a narrow fixation envelope with a shared failure pathway.
Divergent placement disrupts this shared failure mode. By angling screws away from each other, each screw recruits a distinct cortical and trabecular region, creating a broader fixation envelope and multi vector resistance to mechanical loading.
Biomechanical studies across multiple anatomical sites and fixation models have consistently demonstrated that screw trajectory influences pullout resistance. While study designs, bone models, and measurement methods vary, a clear pattern emerges: constructs with optimized divergence perform favorably compared to parallel configurations-particularly in osteoporotic or metaphyseal bone where maximizing fixation pathways is most critical.
Study | Model | Key Finding |
Claes et al., 1995 | Cadaveric screw fixation | Divergence of 30-60° produced 2.5-3× higher pullout strength vs. parallel screws. |
Heetveld et al., 2004 | Distal radius cadaveric model | Divergent locking screws increased pullout strength 1.6-2.2× over parallel constructs. |
Gautier et al., 2005 | Proximal femur cadaveric model | Divergent lag screws demonstrated higher resistance to cut-out and pullout. |
Shen et al., 2012 | Calcaneus cadaveric model | Greater screw divergence improved pullout strength and reduced toggle under cyclic loading. |
Importantly, the literature does not support the notion that more divergence is invariably superior. Excessive angulation beyond anatomical limits can reduce effective bone purchase, compromise screw length, and create suboptimal trajectories. The evidence points toward an optimal range rather than a linear benefit with increasing angulation.
Across cadaveric and biomechanical studies, the optimal divergence angle is generally considered to fall between 15° and 60°, balanced with anatomical and implant constraints specific to each clinical scenario. Surgical judgment must account for fracture morphology, bone quality, and available fixation trajectories.
<15° Minimal benefit; | 15°-60° Maximizes bone purchase; | >60° Risk of cortical breach; |
“In orthopedic fixation, the geometry of placement is as consequential as the implant itself. Optimized divergence is not merely a technique-it is a biomechanical strategy rooted in the fundamental physics of bone-screw interaction.”
Clinical Caveat: Divergence is not a universal solution. In specific anatomical or patient-related scenarios, carefully planned parallel fixation may remain biomechanically preferable. Surgical judgment and pre-operative planning are paramount.

Screw divergence, when applied with anatomical precision and sound biomechanical principles, can meaningfully improve pullout resistance across a range of orthopedic applications. The mechanism is well-established: independent stress cone formation, expanded bone purchase envelopes, and multi-vector resistance to mechanical failure work together to create a fundamentally more robust construct.
The biomechanical evidence-consistently demonstrated across cadaveric models in multiple anatomical regions-supports this principle. However, the critical qualifier is optimized divergence. More angulation is not inherently better. The 15°-60° optimal range, balanced against anatomy, implant design, and bone quality, represents the therapeutic window within which divergence delivers its greatest benefit. Variable-angle locking technology has expanded the practical application of these principles, giving surgeons greater intraoperative flexibility to achieve optimal trajectories in challenging fracture patterns.
References
Disclaimer: This article is intended for educational purposes for healthcare professionals only. It does not constitute professional medical advice, diagnosis, or treatment. All clinical decisions should be made based on individual patient assessment, surgeon judgment, and current evidence-based guidelines.